|
by Sally L. Gaspar, RN2016 Best Practices Summit - Second Place Winner
St Jude Medical Center is a 320 bed, nonprofit Catholic community hospital. A member of St Joseph Hoag Health System, it serves a large senior population and is located in a zip code with twice the percentage of individuals 65 and older as compared with the rest of Orange County.
-
Why did we start the collaboration? With the closure of the St Jude short term SNF aka TCC or Transitional Care Center, the hospital leadership has made it imperative that the hospital partner with local SNFs in order to engage in a stronger collaboration. In addition, the medical center’s strategic goal is to reduce unnecessary transfers to hospital from SNFs through a coordinated hospital-SNF collaboration that improves clinical outcomes through quality of care and reduces costs.
-
How did we start the collaboration? Community partners were chosen. Our bases in choosing the 6 SNFs were as follows: Medicare overall star rating, SNFist care, staffing, quality of care and regulatory compliance. Every month, the 6 partnered SNF and hospital representatives meet and discuss updates, issues and strategies to overcome issues.
Avoidable readmissions are a major financial problem for the nation’s health care. Under the Hospital Readmission Reduction Program, hospitals with high rates of readmissions see a reduction in Medicare payment. The prospect of penalties and reimbursement model changes based on hospital readmission rates.
INTERACT is an evidence-based quality improvement program that has different tools, that focuses on improving the management of acute changes in condition. As a result, hospitalizations are avoided in situations that can be feasibly and safely managed by skilled nursing facilities.
-
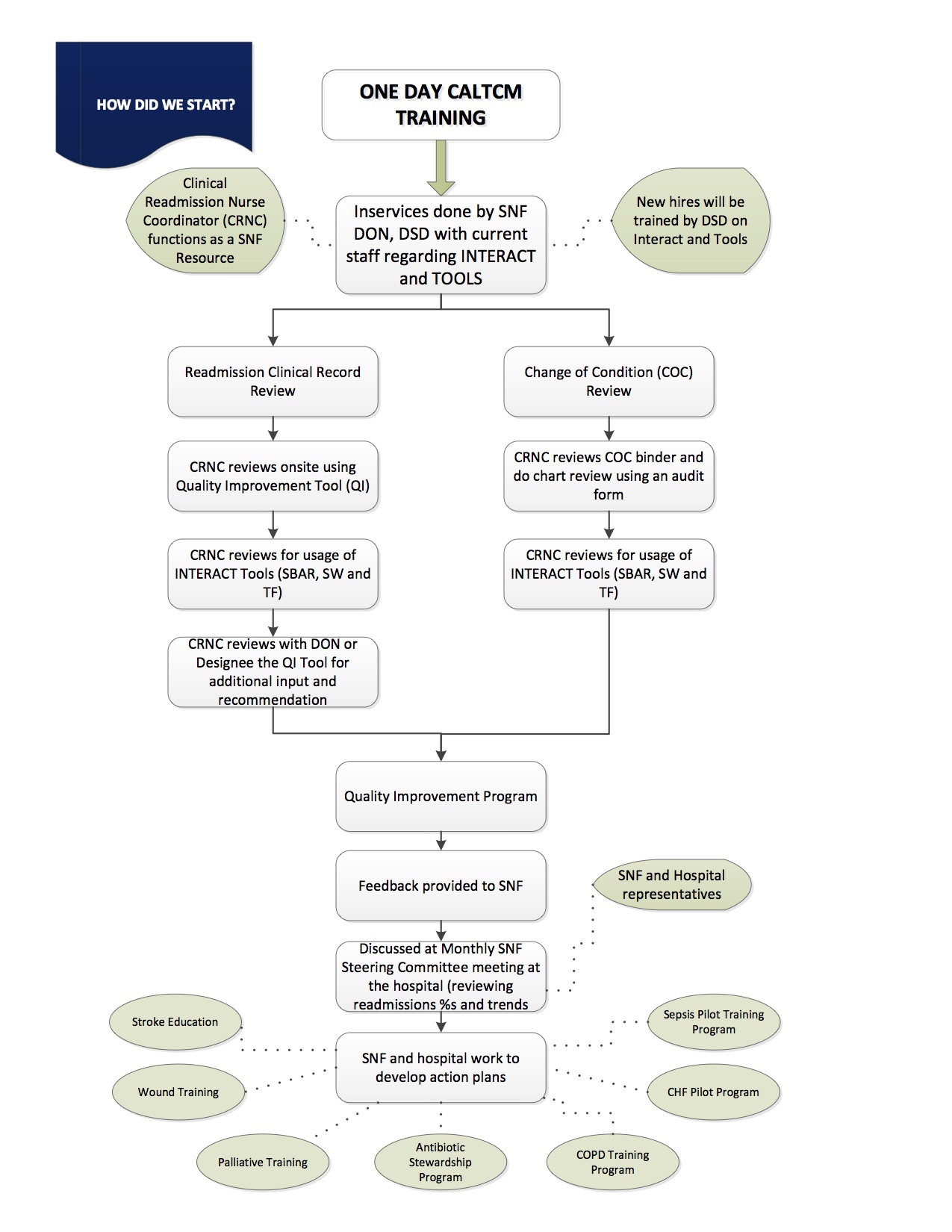
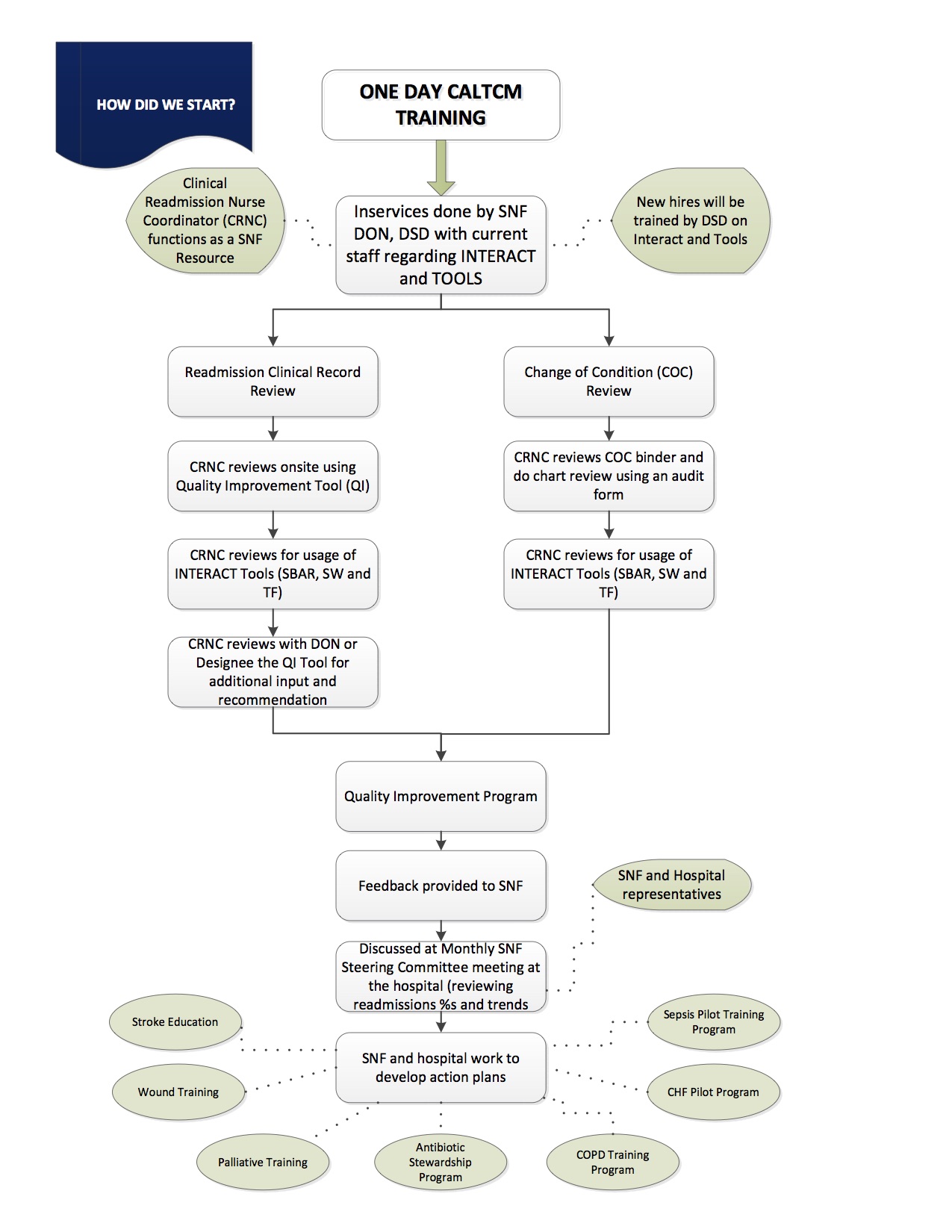
HOW DID WE START INTERACTing? A ONE day CALTCM training done July 2015 at St Jude Medical Center with a goal to train the trainers. Information, gathered from both reviews, is incorporated in the quality improvement program by giving feedback to SNF. It is discussed at monthly SNF steering committee meeting at the hospital. Trends and readmission % are also discussed by SNF and hospital representatives to develop action plans.
-
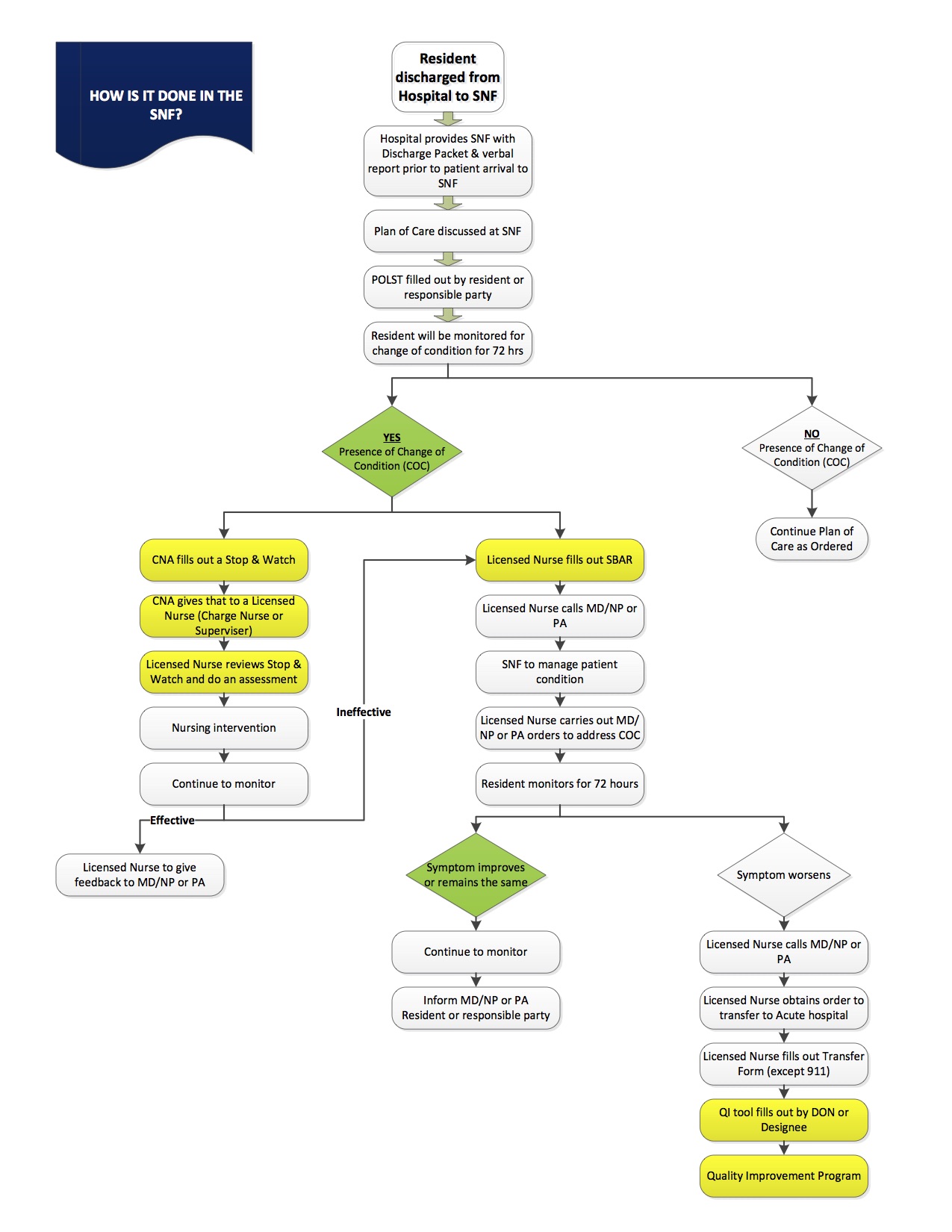
HOW IT IS DONE IN THE SNF? The 6 SNFs have their own clinical operational process. The highlighted yellows are the ones that were added and reemphasized in their system such as SBAR, Stop and watch, QI tool and Transfer form.
-
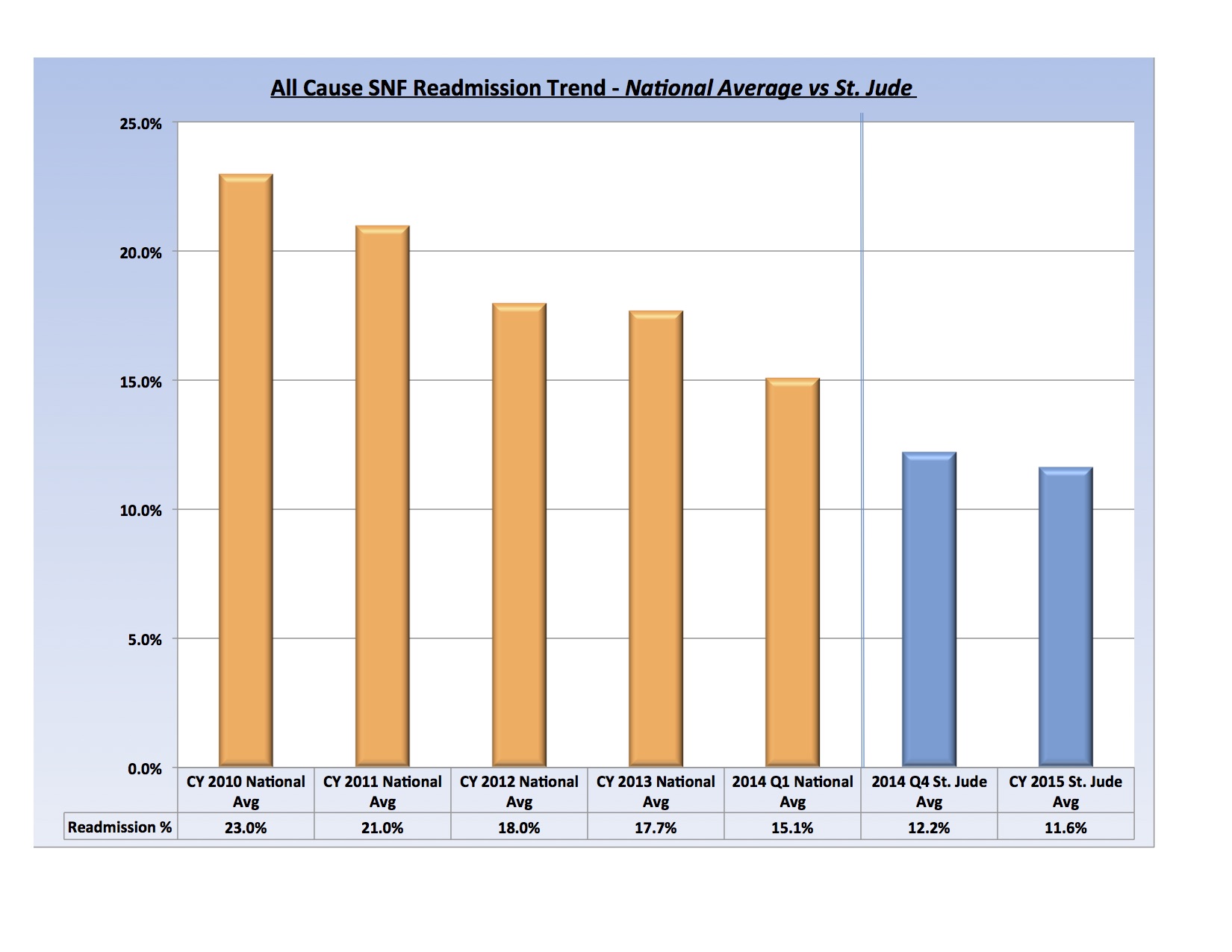
WHAT DOES THIS MEAN? When we started the collaboration and INTERACT planning phase we were at 15% last September 2014. By the end of 2014, we were at 12.2%. Before we started the formal training and implementation of INTERACT, we were at 11.9%. One has to remember that as we were moving forward, we are adding ideas to build momentum. After the July 2015 training, we still continue to modify, plan and implement. By the end of 2015, our SNF readmission rate was down to 11.4%.
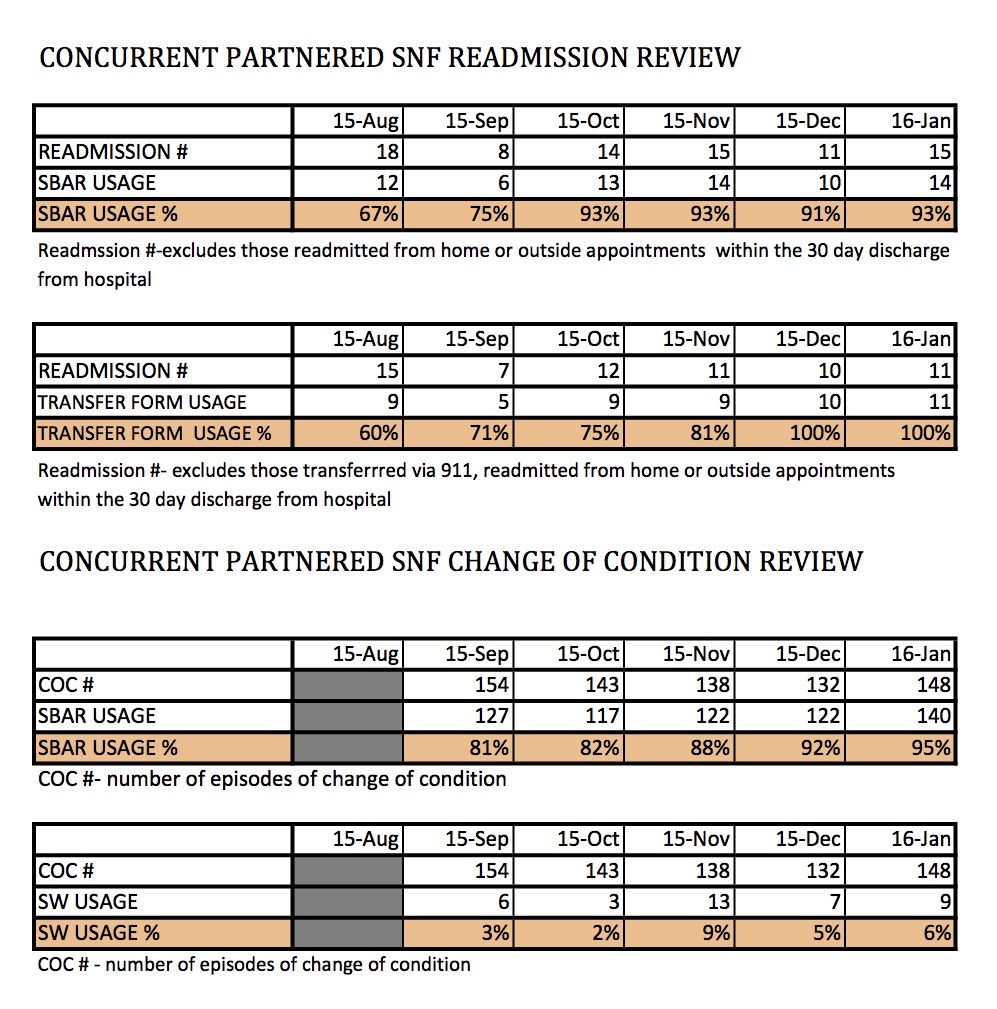
The most important thing I want you to know about this table is to look at the INTERACT tools usage (SBAR, transfer form) in the readmission review and INTERACT tools usage (SBAR, S&W) in the change of condition review. If SNFs use the INTERACT tools (SBAR or S&W or both) appropriately and they are “fully engaged” in using it, more of the patient changes of condition will be managed in the snf and avoid unnecessary transfers.
When Skilled Nursing Facilities are able to prevent unnecessary transfers to hospital and their related complications, they become or continue to become attractive partners for hospitals, health care systems, managed care plans and accountable care organizations. |